 |
Carl Jamieson, owner of the Recent North American Cup winner Up The Credit was an early adopter of Theralase technologies. "I use the Theralase laser on every one of my horses, including Up The Credit,” says Jamieson. “It's great for knees, hocks, tendons and especially sesmoiditis. I've never seen complete healing so clean and fast.”
Blair Burgess, trainer of Blue Porche winner of the 2011 Goodtimes Trot also uses Theralase technologies to address inflammation in his equine athletes. “I definitely noticed decreased inflammation in a shorter amount of time,” said Burgess. “All my other treatment protocols had been followed as per usual and we had never seen healing at that speed before.”
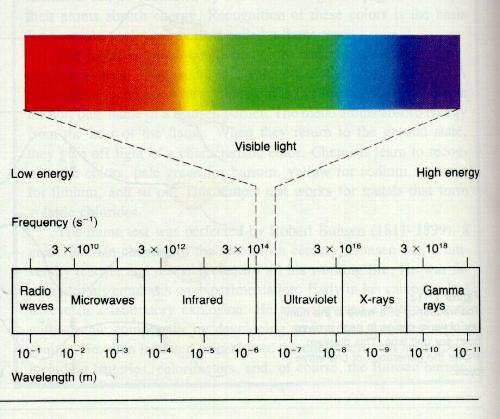
Light therapy has been shown in over 40 years of independent research worldwide to deliver powerful therapeutic benefits to living tissues and organisms. Both visible red and infrared light have been shown to effect at least 24 different positive changes at a cellular level. Visible red light, at a wavelength of 660 nanometers (nm – 1 nanometer is equal to one billionth of a meter), penetrates tissue to a depth of about 8-10 mm. It is very beneficial in treating problems close to the surface such as wounds, cuts, scars, trigger and acupuncture points and is particularly effective in treating infections. Infrared light (904nm) penetrates to a depth of about 30-40 mm which makes it more effective for bones, joints, deep muscle, etc.
The diverse tissue and cell types in the body all have their own unique light absorption characteristics; that is, they will only absorb light at specific wavelengths and not at others. For example, skin layers, because of their high blood and water content, absorb red light very readily, while calcium and phosphorus absorb light of a different wavelength. Although both red and infrared wavelengths penetrate to different depths and affect tissues differently, their therapeutic effects are similar.
Depth of penetration is defined as the depth at which 60% of the light is absorbed by the tissue, while 40% of the light will continue to be absorbed in a manner that is less fully understood. Treating points with Light can have a dramatic effect on remote and internal areas of the body through the stimulation of nerves, acupuncture and trigger points that perform a function not unlike transmission cables.
At this time, research has shown no side effects from this form of therapy. Occasionally, one may experience an increase in pain or discomfort for a short period of time after treating chronic conditions. This occurs as the body reestablishes new equilibrium points following treatment. It is a phenomenon that may occur as part of the normal process of recovery.
Light therapy has also been given the name " phototherapy". A study done by the Mayo Clinic in 1989 suggests that the results of light therapy are a direct effect of light itself, generated at specific wavelengths, and are not necessarily a function of the characteristics of coherency and polarization associated with lasers. In a study entitled Low-Energy Laser Therapy: Controversies and New Research Findings, Jeffrey R. Basford, M.D. of the Mayo Clinic’s Department of Physical Medicine and Rehabilitation, suggests that the coherent aspect of laser may not be the source of its therapeutic effect. He states "firstly, the stimulating effects (from therapeutic light) are reported following irradiation with non-laser sources and secondly, tissue scattering, as well as fiber optic delivery systems used in many experiments rapidly degrade coherency . . . Thus any effects produced by low-energy lasers may be due to the effects of light in general and not to the unique properties of lasers. This view is not difficult to accept when it is remembered that wave-length dependent photobiochemical reactions occur throughout nature and are involved in such things as vision, photosynthesis, tanning and Vitamin D metabolism. In this view, laser therapy is really a form of light therapy, and lasers are important in that they are convenient sources of intense light at wavelengths that stimulate specific physiological functions (Lasers in Surgery and Medicine9:1-5, Mayo Clinic, Rochester, Minnesota, 1989).
LED’s and LASERS are no more than convenient devices for producing electromagnetic radiation at specific wavelengths, and in addition to the one already cited, several other studies establish that it is the light itself at specific wavelengths that is therapeutic in nature and not the machine which produced it. For example, Kendric C. Smith at the Department of Radiation Oncology, Stanford University School of Medicine, concludes in an important article entitled The Photobiological Effect of Low Level Laser Radiation Therapy (Laser Therapy, Vol. 3, No. 1, Jan - Mar 1991) that "1) Lasers are just convenient machines that produce radiation. 2) It is the radiation that produces the photobiological and/or photophysical effects and therapeutic gains, not the machines. 3) Radiation must be absorbed to produce a chemical or physical change, which results in a biological response."
The equation between the machine and the biological response is a common error often made by those who wish to promote the commercial interests of low-energy laser technology. Light radiation must be absorbed to produce a biological response. All biological systems have a unique absorption spectrum which determines what wavelengths of radiation will be absorbed to produce a given therapeutic effect. The visible red and infrared portions of the spectrum have been shown to have highly absorbent and unique therapeutic effects in living tissues.
The following are definitions of commonly used terms used in connection with the use of therapeutic light devices:
| 1) Visible Light: light that is within the visible spectrum, 400nm(violet) to 700nm(red) 2) Infrared Light: light in the invisible spectrum below red, from 700nm to 2,000nm 3) Frequency: number of cycles per second measured in Hertz 4) Coherency: wavelengths of light traveling in phase with one another 5) Monochromaticity: light that is of one color, or one wavelength 6) Collimation: light focused in a beam, maintaining a constant diameter regardless of its distance from the object or surface at which it is directed 7) Nanometer (nm): a unit of measure of wavelength of light (one billionth of a meter) 8) Nanosecond: one billionth of a second 9) Joule (J): unit used to measure the energy delivered 10) Watts (w) and milliwatts (mw, 1/ 1000th of a watt): units used to measure the power capability 11) Peak power output: the maximum output of power, measured in milliwatts and watts 12) Average power: amount of power actually delivered in a given period of time 13) Duty cycle: the amount of time the light is actually on during a given period of time |
Lasers are of two principal types, "hot" and "cold", and they are distinguished by the amount of peak power they deliver. "Hot" lasers deliver power up to thousands of watts. They are used in surgery because they can make an incision that is very clean with little or no bleeding and because the laser cauterizes the incision as it cuts. They are also used in surgery that requires the removal of unhealthy tissue without damaging the healthy tissue that surrounds it. . "Cold" lasers produce a lower average power of 100 milliwatts or less. This is the type of laser that is used for therapeutic purposes and it is typically, although not always, pulsed. The light is actually on for only a fraction of a second because it is pulsed (turned on and off) at so many pulses per second. Pulsation results in an average power output that is very low compared to the maximum or peak output. Hence, most therapeutic lasers produce a high peak but low average power output. Therapeutic laser light is generally either visible (red, in most cases) or invisible (infrared). However, most therapeutic lasers operate at 904 nm which is an infrared light.
Light Emitting Diodes (LEDs) are another form of light therapy that is a relatively recent development of the laser industry. LEDs are similar to lasers inasmuch as they have the same healing effects but differ in the way that the light energy is delivered. A significant difference between lasers and LEDs is the power output. The peak power output of LEDs is measured in milliwatts, while that of lasers is measured in watts. However, this difference when considered alone is misleading, since the most critical factor that determines the amount of energy delivered is the duty cycle of the device.
LED devices usually have a 50% duty cycle. That is, the LED pulse is "on" for 0.5 seconds and "off" for 0.5 seconds versus the 2 ten-millionths of a second burst from laser at 1 cycle per second (1 herz). Moreover, LED is "on" 50% of the time and "off" 50% of the time regardless of what frequency setting (pulses per second) is used.
In the majority of lasers on the market, the energy output varies with the frequency setting: the lower the frequency, the lower the output. In the BioScan system on the contrary, the output is constant regardless of frequency. Even in the case of lasers that claim a peak output of 10 watts, because of the very short duty cycle, the average output at the highest frequencies is of the order of about 10 milliwatts. At the lower frequencies, however, the average output plummets into the range of microwatts (1 microwatt = 1000th of 1 milliwatt).
LEDs do not deliver enough power to damage the tissue, but they do deliver enough energy to stimulate a response from the body to heal itself. With a low peak power output but high duty cycle, the LEDs provide a much gentler delivery of the same healing wavelengths of light as does the laser but at a substantially greater energy output. For this reason, LEDs do not have the same risk of accidental eye damage that lasers do.
Moreover, LEDs are neither coherent nor collimated and they generate a broader band of wavelengths than do the single-wavelength laser. Non-collimation and the wide-angle diffusion of the LED confers upon it a greater ease of application, since light emissions are thereby able to penetrate a broader surface area. Moreover, the multiplicity of wavelengths in the LED, contrary to the single-wavelength laser, may enable it to affect a broader range of tissue types and produce a wider range of photochemical reactions in the tissue. /stronga
If LED disperses over a greater surface area, this results in a faster treatment time for a given area than laser. The primary reason that BioScan chose the LEDs over lasers is that LEDs are safer, more cost effective, provide a gentle but effective delivery of light and a greater energy output per unit of surface area in a given time duration. They are offered in combinations of visible red light at 660nm and infrared light at from 830nm to 930nm, with 880nm as their average.
Light therapy can:
|
References
The Photobiological Basis of Low Level Laser Radiation TherapyThe Photobiological Basis of Low Level Laser Radiation Therapy, Kendric C. Smith; Stanford University School of Medicine; Laser Therapy, Vol. 3, No. 1, Jan - Mar 1991
Low-Energy Laser Therapy: Controversies Research Findings, Jeffrey R. Basford MD; Mayo Clinic; Lasers in Surgery and Medicine 9, pp. 1-5 (1989)
New Biological Phenomena Associated with Laser Radiation , M.I. Belkin U. Schwartz; Tel-Aviv University; HealthPhysics, Vol. 56, No. 5, May 1989; pp. 687-690
Macrophage Responsiveness to Light Therapy, S Young PhD, P Bolton BSc, U Dyson PhD, W Harvey PhD, C Diamantopoulos BSc; London: Lasers in Surgery and Medicine, 9; pp. 497-505 (1989)
Photobiology of Low-Power Laser Effects, Tina Karu PhD; Laser Technology Centre of Russia; Health Physics, Vol. 56, No. 5. May 89, pp. 691-704
A Review of Low Level Laser Therapy, S Kitchen MSCMCSP C Partridge PhD; Centre for Physiotherapy Research, King's College London Physiotherapy, Vol. 77, No. 3, March 1991Systemic Effects of Low-Power Laser Irradiation on the Peripherial Central Nervous System, Cutaneous Wounds a
Burns, S Rochkind MD, M Rousso MD, M Nissan PhD, M Villarreal MD, L Barr-Nea PhD. DG Rees PhD, Lasers in Surgery and Medicine, 9; pp. 174-182 (1989)
Use of Laser Light to Treat Certain Lesions in Standardbreds, L.S McKibbin DVM, D Paraschak BSc., MA; Mod Veterinary Practice, March 1984, Sec. 3, p. 13
Low Level Laser Therapy: Current Clinical Practice In Northern Ireland, GD Baxter BSc, AJ Bet, MA,,JM AtienPhD, J Ravey PhD; Blamed Research Centre University Ulster Physiotherapy, Vol. 77, No. 3, March 1991
The Effects of Low Energy Laser on Soft Tissue in Veterinary Medicine, LS McKibbin R Downie; The Acupuncture Institute, Ontario Canada; J. Wiley Sons
A Study of the Effects or Lasering of Chronic Bowed Tendons, Wheatley, LS McKibbin DVM, and DM Paraschak Bsc MA; Lasers in Surg Medicine, Vol. pp. 55-59 (1983) Scc 3
Lasers and Wound Healing, Albert J. Nemeth, MD; Laser and Dermatology Center, Clearwater FL, Dermatologic Clinics, Vol.. 11 #4, 1993
Low Level Laser Therapy: A Practical Introduction, T. Ohshiro RG Caiderhead, Wiley and Sons
Low Reactive-Level Laser Therapy: A Practical Application, T. Ohshiro;Book:Wiley and Sons
Laser Biostimulation of Healing Wounds: Specific Effects and Mechanisms of Action,Chukuka S Enwemeka, PhD; Assistant Professor of Physical Therapy - U. of Texas, Health Science Center, San Antonio, TX; The Journal of Orthopaedic Sports Physical Therapy, Vol. 9. No.10, 1988
Effect of Helium-Neon and Infrared Laser Irradiation on Wound Healing in Rabbits, B Braverman, PhD; R McCarthy. Pharmd, A Lyankovich, MD; D Forde, BS, M Overfield, BS and M Bapna, PhD; Rush- Presbyterian-St. Luke's Medical Center; University of Illinois, Lasers in Surgery and Medicine 9:50-58 (1989)
Bone Fracture Consolidates Faster With Low-Power Laser, MA Trelles, MD and E Mayayo, MD, Barcelona, Spain; Lasers in Surgery Med. 7:36-45 (1987)
Wound Management with Whirlpool and Infrared Cold Laser Treatment,P Gogia; B Hurt and T Zim; AMI-Park Plaza Hospital, Houston TX, Physical Therapy, Vol. 68, No. 8, August 1988
Effects of Low-Level Energy Lasers on the Healing of Full-Thickness Skin Defects, J Surinchak. MA; M Alago, BS,, R Bellamy, MD; B Stuck, MS and M Belkin, MD; Lettennan Army Institute of Research. Presido of San Fransico, CA; Lasers in Surgery Medicine, 2:267-274 (1983)
Biostimulation of Wound Healing by Lasers: Experimental Approaches in Animal Models and in Fibroblast Cultures, RP Abergel, MD; R Lyons. MD; J Castel, MS, R Dwyer. MD and i Uitlo. MD, PhD; Harbor UCLA Medical Center. CA: J Dennatol. Surgery Oncol., 13:2 Feb. 1987
Effects of Low Energy Laser on Wound Healing In a Porcine Model, J Hunter, MD; L Leonard, MD; R Wilsom MD; G Snider, MD and J DLxon, MD; Department of Surgery, University of Utah Medical Center, Salt Lake City UT, Lasers in Surgery Med. 3:285-290, 84
Effect of Laser Rays on Wound Healing, E Mester, MD; T Spiry, MD; B Szende. MD and J Tola; Semmelweis Medical Univ. Budapes, The American Journal of Surgery. Vol 122, Oct 1971
Low Level Laser Therapy in the United Kingdom, Kevin C Moore, MD; The Royal Oldham Hospital, Oldhant, UK
Effects of Skin-Contact Monochromatic Infrared Irradiation on Tendonitis, Capsulitis and Myofascial Pain, T.L Thomassoi DDS, 19th Annual Scientific Meeting, American Academy of Neurological Orthopaedic Surgeons, Aug. 27-30, 1995 Facial Pain/TMJ Centre, Denver, CO
For further information please call 1-866-843-5273 or visit www.theralase.com


